It is necessary to know something about the anatomy of the fetus and the maternal pelvis in order to understand how shoulder dystocia comes about and how it causes the injuries it does.
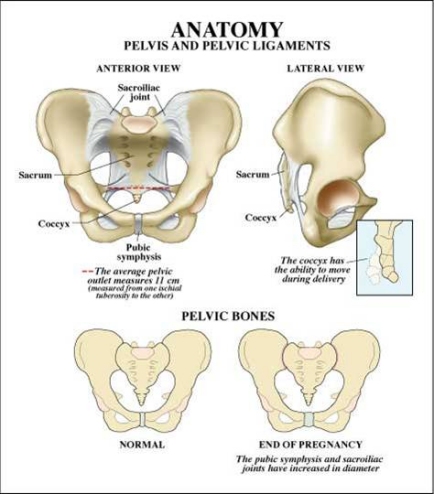
As the accompanying diagram shows, the maternal pelvis is composed of a series of bones forming a circle protecting the pelvic organs. The front-most bone is the symphysis pubis. It is on this structure that a baby's anterior shoulder gets caught during a delivery complicated by shoulder dystocia. The bone at the back of the maternal pelvis is the sacrum. Because of its shape, it generally serves as a slide over which a baby's posterior shoulder can descend freely during labor and delivery. However sometimes a baby’s posterior shoulder can get caught on its slight projection into the pelvis. The side walls of the maternal pelvis, although very important in determining how smoothly the process of labor will go, usually do not contribute to shoulder dystocia.
click on
image to view larger image
In normal vaginal deliveries the head of the baby, called the "vertex", emerges first. During labor, the soft, mobile bones of the fetal head can overlap and the head as a whole can "mould"—go from perfectly round to more pointed and narrower. This facilitates the fetal head fitting into and through the maternal pelvis. The baby's shoulders, likewise being flexible, usually follow the delivery of the baby's head quickly and easily. But for this to happen, the axis of the fetal shoulders must descend into the maternal pelvis at an angle oblique to the pelvis's anterior-posterior dimension. This position affords the shoulders the most room for their passage. If instead the shoulders line up in a straight front-to-back orientation as they are about to emerge from the mother's pelvis, there will often be insufficient room for them to squeeze through. The back of the mother's pubic bone then forms a shelf upon which the baby's anterior shoulder gets caught. If this happens, the shoulders cannot deliver and a shoulder dystocia results.
As previously mentioned, shoulder dystocia can also occur if the posterior shoulder of a baby gets caught on its mother's sacrum. This is a far less common cause of shoulder dystocia. The sacrum, having only a slight protrusion, is far less likely to impede the descent of the baby's posterior shoulder than is the mother’s pubic bone to block passage of the baby’s anterior shoulder.
As can be readily appreciated, it is the relative sizes of the fetal head, shoulders, and chest compared to the shape and size of the maternal pelvis that determine how smoothly a delivery will go. Usually it is the fetal head that has the largest fetal dimensions. Thus if the head can pass through the maternal pelvis without difficulty, the rest of the baby usually follows easily. However, when the dimensions of the fetal shoulders or chest rival those of its head—such as in an especially large baby or a baby of a mother with diabetes-- the chances of a shoulder dystocia occurring are much increased. Since larger babies, whether of diabetic mothers or not, are more likely to "get stuck", much of the work in the field of shoulder dystocia has been targeted at attempting to predict which babies will be larger than normal, especially when their mothers are diabetic.
Except in extraordinary circumstances, once the fetal head and shoulders have been delivered the remainder of the fetal trunk and legs slide out easily. Such extraordinary circumstances preventing easy delivery of the fetal body might occur when:
- A fetus has a large abdominal or lower back tumor,
- The umbilical cord is wrapped tightly around the baby's neck, or
- There is a severe constriction of the uterine muscle -- "contraction ring" -- trapping the baby in the uterus.
The above applies only to vertex (headfirst) deliveries. Breech deliveries, where the fetal legs and buttocks emerge first from the vagina, can also result in injury to the brachial plexus, producing the sorts of injuries discussed above. However, since vaginal breech deliveries are known to produce a higher rate of neonatal morbidity and even mortality, most breech babies in the United States are now delivered by cesarean section.
next >>

